JP
Dr. Jayen Patel, MD
Board-Certified Pain Management Physician · Founder, SEVA Healthcare
13 min read
Key Takeaways
- Up to 25% of people with diabetes
develop painful diabetic neuropathy (PDN). It is one of the most common — and most undertreated — chronic pain conditions in Tulsa.
- Standard PDN medications (gabapentin, pregabalin, duloxetine) help fewer than half
of patients meaningfully and often come with side effects.
- Spinal cord stimulation is now FDA-approved
specifically for painful diabetic neuropathy. Multiple 2023–2024 trials
show high-frequency 10 kHz SCS produces significant, durable pain relief.
- A 2025 retrospective cohort study in The Lancet eClinicalMedicine
linked SCS for PDN with reduced amputations, lower mortality, and fewer major adverse cardiovascular events.
- SEVA Healthcare offers full PDN evaluation and treatment at both Midtown Tulsa
and South Sheridan, with same-week appointments.
If you have diabetes and you live with burning, tingling, or sharp shooting pain in your feet — especially at night — you are dealing with one of the most common and life-disrupting forms of chronic pain. And in 2026, the treatment landscape for painful diabetic neuropathy looks very different than it did just five years ago.
This guide explains what painful diabetic neuropathy is, why medications often fall short, and what the latest FDA-approved treatments — including high-frequency spinal cord stimulation — can do for Tulsa patients.
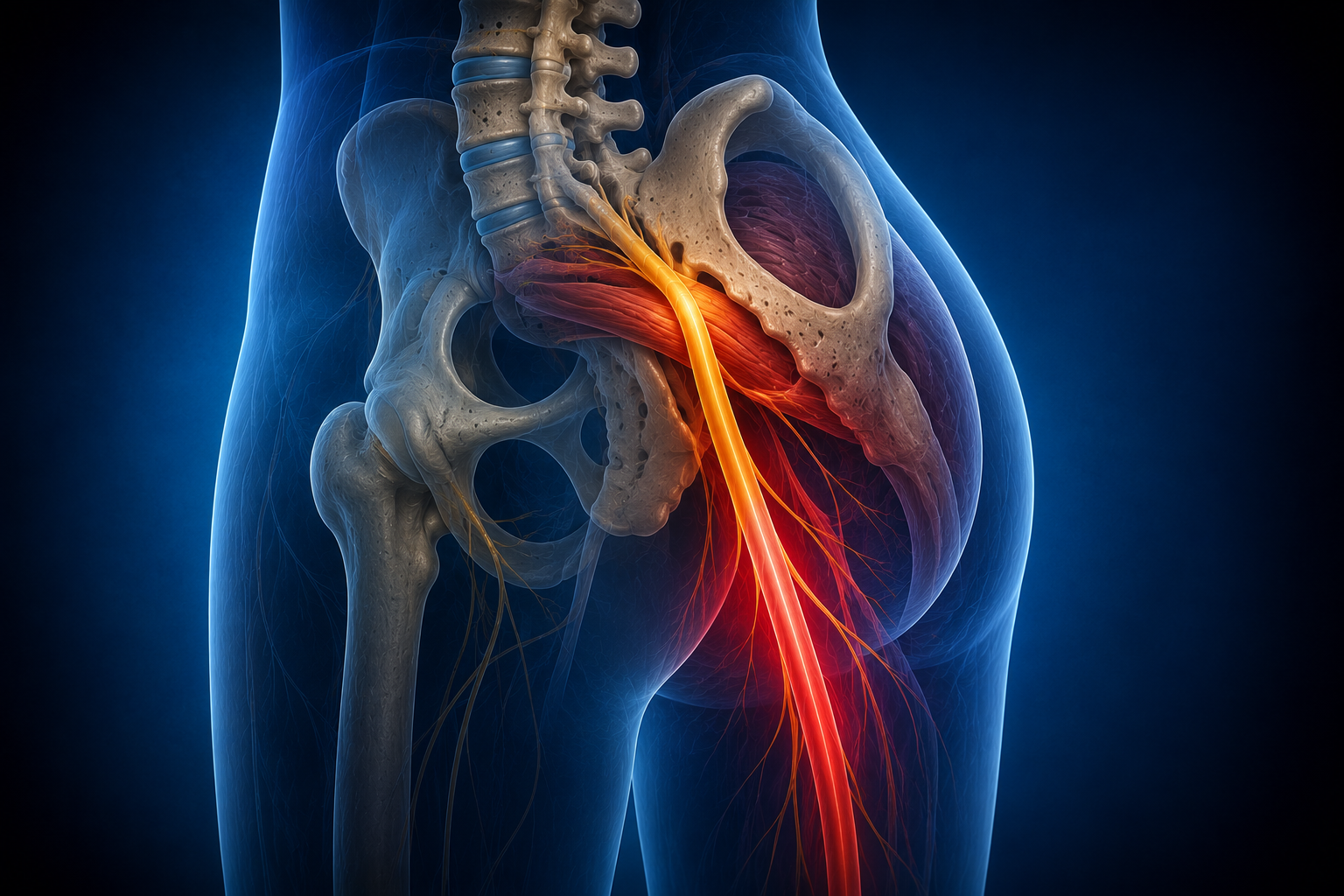
What is painful diabetic neuropathy?
Painful diabetic neuropathy (PDN) is nerve damage caused by long-term high blood sugar. It most often affects the longest nerves first — the ones reaching to the feet — and then progresses up the legs and sometimes into the hands.
Typical symptoms include:
- Burning pain in the feet, often worse at night.
- Tingling, pins-and-needles sensation.
- Shooting or stabbing pain.
- Hypersensitivity to touch (even bedsheets can hurt).
- Numbness alongside the pain — you may feel less sensation but still have constant burning.
- Loss of balance, especially walking in the dark.
In plain language
The nerves in your feet are damaged and misfiring. Sometimes they send pain signals when nothing is wrong. Sometimes they send the wrong signal entirely — numbness in one place and burning in another. The goal of treatment isn’t just to dull the pain — it’s to retrain how those nerve signals travel.
Why standard medications often fall short
The first-line medications for PDN are well known:
- Gabapentin and pregabalin (Lyrica)
— quiet down the misfiring nerves.
- Duloxetine (Cymbalta)
— an SNRI that modulates pain processing.
- Tricyclic antidepressants
— older but effective for some patients.
- Topical agents
— capsaicin, lidocaine patches.
These help, but the published response rates are honest: fewer than half
of PDN patients get clinically meaningful relief from any single agent, and side effects (drowsiness, weight gain, dizziness) drive many people off them. For patients who don’t respond to medication — or can’t tolerate it — it used to mean living with the pain. That has changed.
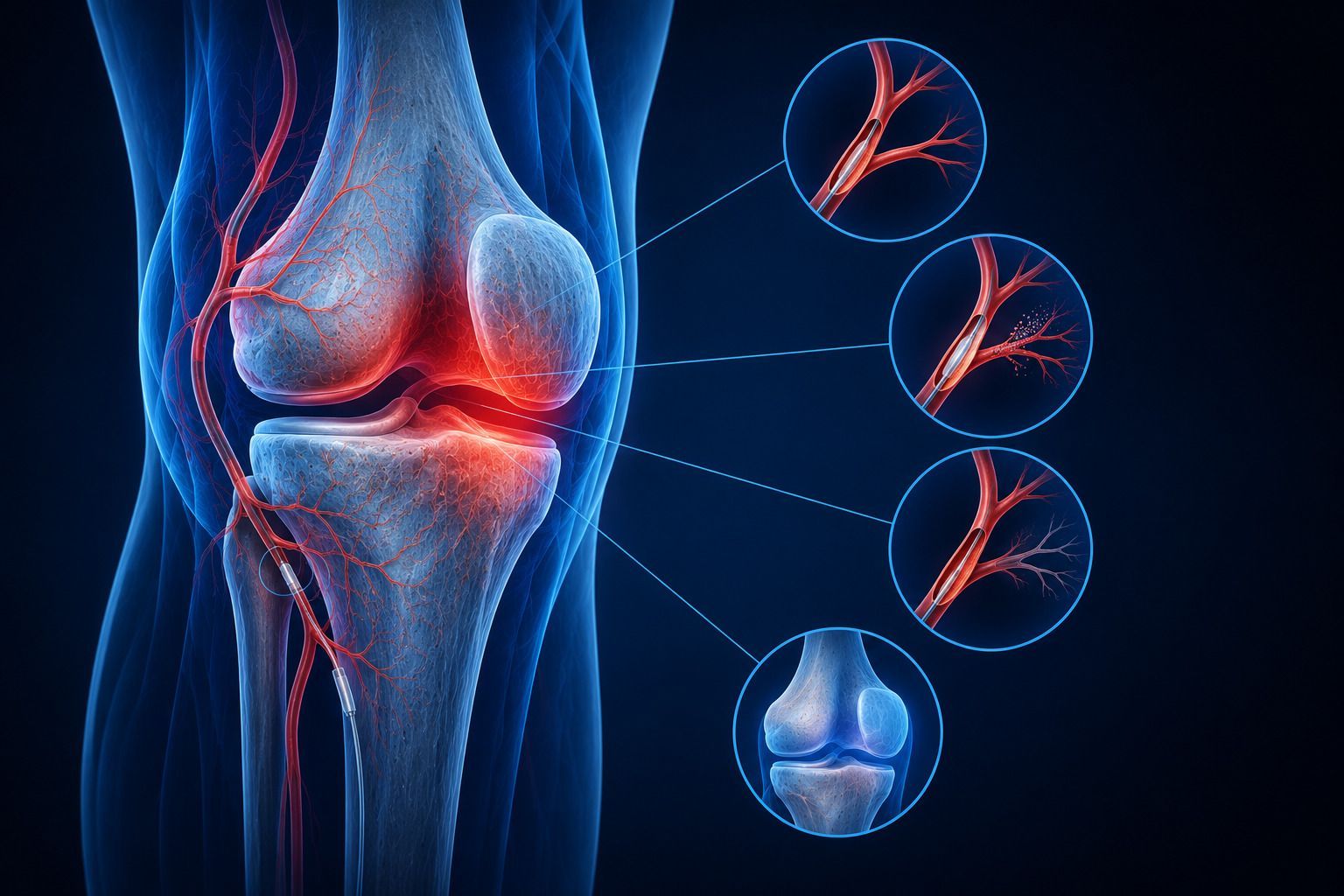
Spinal cord stimulation is FDA-approved for painful diabetic neuropathy
In 2021, the FDA approved spinal cord stimulation specifically for refractory painful diabetic neuropathy — the first time SCS had a dedicated indication for this condition. Modern SCS uses a small device, implanted near the spine, that delivers gentle electrical signals to interrupt pain transmission before it reaches the brain.
The most important advance for PDN has been high-frequency 10 kHz SCS, which delivers therapy without the tingling (paresthesia) of older systems — making it more comfortable and often more effective.
What the evidence shows:
- Significant pain reduction
— the pivotal SENZA-PDN trial showed sustained >50% pain relief in the majority of patients at 12 and 24 months.
- Quality of life improvements
— better sleep, reduced sensitivity, improved walking tolerance.
- Beyond pain
— a 2025 retrospective cohort study published in The Lancet eClinicalMedicine
reported that PDN patients treated with SCS had lower rates of amputation, lower all-cause mortality, fewer major adverse cardiovascular events, and lower infection risk
compared to matched patients managed without SCS.
Honest note from Dr. Patel
No treatment is right for everyone. SCS requires a 5–7 day trial period before permanent implant — specifically so we can see whether your
nerves respond. If the trial doesn’t produce meaningful relief, we don’t move forward with the implant. That’s the protocol, and it’s the right one.
The treatment pathway at SEVA Healthcare Tulsa
1
Full evaluation
A thorough history, exam (including monofilament and vibration testing), and review of your diabetes control. We also confirm the diagnosis — not every burning-feet sensation is PDN.
2
Optimize medical management
If you haven’t tried gabapentin, pregabalin, or duloxetine, that’s usually step one. If you have tried them and they didn’t help — or weren’t tolerated — we move on.
3
Peripheral nerve blocks & sympathetic blocks
Lumbar sympathetic blocks can be diagnostic and therapeutic for severe burning lower-extremity pain. They also tell us whether SCS is likely to help.
4
SCS trial
A 5–7 day outpatient trial of high-frequency 10 kHz SCS. Temporary leads are placed; you go home, use the device normally, and we measure whether your pain genuinely improves.
5
Permanent SCS implant if the trial works
If the trial reduces your pain meaningfully (typically >50%), we proceed to the permanent system. The implant is outpatient. Recovery is days, not weeks.
6
Ongoing diabetes coordination
We coordinate with your primary care physician or endocrinologist throughout. Better glucose control improves nerve health over time — the two parts of the plan reinforce each other.
Treatment options compared
| Option |
Typical response |
Notes |
| Gabapentin / Pregabalin |
~30–45% with meaningful relief |
First-line; side effects common |
| Duloxetine |
~30–40% response |
SNRI; may help mood too |
| Topical capsaicin / lidocaine |
Modest in isolation |
Useful adjunct |
| Lumbar sympathetic block |
Diagnostic + temporary relief |
Bridge to SCS |
| 10 kHz SCS |
Majority >50% relief at 12 months |
FDA-approved for PDN |
| Peripheral nerve stimulation |
Focal nerve targets |
Useful for localized neuralgia |
Where to be seen for diabetic neuropathy in Tulsa
Frequently asked questions
Can spinal cord stimulation reverse my neuropathy?
SCS doesn’t repair the damaged nerves — it interrupts the pain signals before they reach your brain. Some patients also report improved sensation; the mechanism for that is still being studied.
Is SCS covered by Medicare for diabetic neuropathy?
Yes. Since FDA approval for PDN, Medicare and most major commercial plans cover SCS for diabetic neuropathy that has not responded to conservative therapy.
How long is the SCS trial?
Typically 5–7 days. You go home with the trial leads in place, use the device during normal daily activities, and we evaluate whether your pain is meaningfully reduced.
Will I still need my diabetes medications?
Yes. SCS treats the pain. Good glucose control still matters for preventing further nerve damage, cardiovascular complications, and other diabetes-related problems. We work alongside your PCP or endocrinologist.
What if I can’t have surgery?
SCS implant is minimally invasive — outpatient, with small incisions. Many patients who cannot have major surgery can still have SCS. We evaluate medical fitness during your initial consultation.
Related articles from SEVA Healthcare
Take the next step
See a board-certified pain doctor for diabetic neuropathy in Tulsa
Same-week consultations at Midtown and South Sheridan. We will review your medications, exam, and imaging — and explain whether SCS, peripheral nerve stimulation, or another option is right for you.
OK: (918) 935-3240 · sevahealthcare.com
Informational only; not medical advice. Written by Dr. Jayen Patel, MD. Medically reviewed by Dr. Amit Mirchandani, MD. Last updated May 19, 2026.