AM
Dr. Amit Mirchandani, MD
Double Board-Certified Anesthesiology & Pain Medicine · Yale + Rush trained
13 min read
Key Takeaways
- Sciatica isn’t a diagnosis — it’s a symptom. Real treatment starts with identifying the specific structure
compressing the nerve.
- About 80% of acute sciatica improves with conservative care in 6–12 weeks. If yours hasn’t, you don’t need to wait longer — you need a different evaluation.
- A 2025 meta-analysis of 72 randomized controlled trials with 7,701 patients
confirmed that transforaminal epidural steroid injections provide meaningful relief for sciatica from disc herniation, lasting up to 12 months in many patients.
- For sciatica that persists after injections, options include nerve root pulsed radiofrequency, peripheral nerve stimulation, and spinal cord stimulation
— not necessarily surgery.
- SEVA Healthcare treats sciatica patients at Lewisville (North Dallas)
and Rowlett (East Dallas)
— with same-week appointments.
If you have been dealing with sharp, shooting pain down your leg for weeks or months, and physical therapy, anti-inflammatories, or chiropractic adjustments haven’t fixed it, you are likely past the point where waiting will help. The right step is not necessarily surgery — but it is a precise diagnosis of what is actually compressing your nerve.
This guide explains what sciatica really is, why generic treatment so often fails, what the latest evidence says about epidural injections, and what to do when conservative care has run out of road. Written for patients in Dallas, Plano, Lewisville, Rowlett, Frisco, Garland, and across the DFW metroplex.
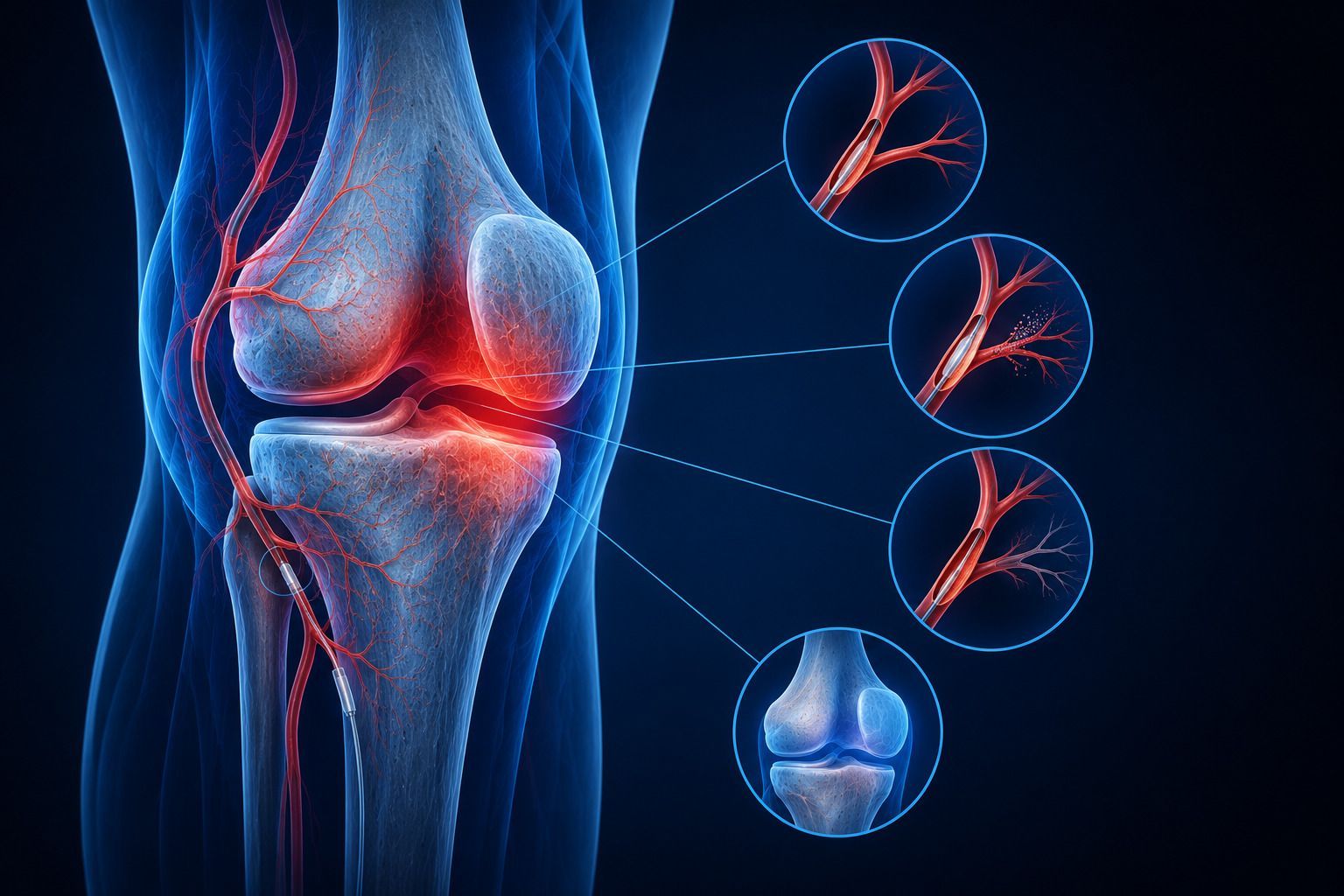
Sciatica is a symptom, not a diagnosis
“Sciatica” describes pain in the distribution of the sciatic nerve
— typically from the low back down through the buttock, the back of the thigh, and sometimes into the calf or foot. But that pain can come from several distinct causes:
- Lumbar disc herniation
— the most common cause. A piece of disc material presses on the nerve root as it leaves the spine (typically L4-L5 or L5-S1).
- Lumbar spinal stenosis
— narrowing of the spinal canal compresses multiple nerve roots. More common in patients over 60.
- Foraminal narrowing
— the small opening where the nerve exits is narrowed by bone spurs or disc degeneration.
- Piriformis syndrome
— the sciatic nerve gets irritated by the piriformis muscle in the buttock. Often missed on MRI.
- Sacroiliac joint pain
— can mimic sciatica with pain into the buttock and posterior thigh.
Honest note from Dr. Mirchandani
A lot of Dallas patients arrive at our clinic having been treated for “sciatica” for months — without anyone identifying which of the five causes above is actually responsible. The treatment for L5 radiculopathy from a disc is different from the treatment for piriformis syndrome. If your diagnosis hasn’t been narrowed down to a specific anatomical structure, your treatment plan can’t be either.
When conservative care has had a fair chance
Most acute sciatica improves with 6–12 weeks of conservative care: anti-inflammatories, physical therapy focused on neural mobilization and core stabilization, and time. If you’ve done all of that and pain persists, that’s your signal it is time for a precise diagnosis and a targeted intervention. Specifically, see a pain specialist if:
- Pain has lasted more than 6 weeks
despite PT and medication.
- You have progressive weakness
in the leg or foot.
- You have numbness or tingling
that is getting worse.
- Sciatica is interfering with sleep, work, or driving.
- An MRI shows a disc herniation but you don’t want surgery without trying everything else first.
Emergency signs — do not wait
If you experience new loss of bladder or bowel control, saddle numbness, or rapidly progressive leg weakness, go to an emergency room immediately. These can indicate cauda equina syndrome, which is a surgical emergency.
What an interventional pain specialist does next
1
A real exam, not just a chart review
Strength testing, reflexes, sensory testing, straight leg raise, FABER and Gaenslen for SI joint, palpation of the piriformis. A pain specialist should be able to clinically narrow the cause before imaging is even considered.
2
Imaging review with intent
We read your MRI looking for the structure that explains your specific symptoms — not just the worst-looking finding. An MRI of an asymptomatic 50-year-old will often show several disc bulges; the question is which ones matter.
3
Diagnostic / therapeutic injection
A transforaminal epidural steroid injection — performed under live fluoroscopy — both confirms the diagnosis and provides relief. The 2025 meta-analysis of 72 RCTs / 7,701 patients showed significant pain reduction and functional improvement at 6 weeks and out to 12 months.
4
Pulsed radiofrequency or PNS if needed
For patients who respond to injections but the relief is short-lived, pulsed radiofrequency near the dorsal root ganglion can extend relief. Peripheral nerve stimulation is another option for focal sciatic pain.
5
Spinal cord stimulation for refractory sciatica
For sciatica that doesn’t respond to injections — particularly post-surgical / failed back surgery patients — spinal cord stimulation
can provide durable relief, especially with modern 10 kHz high-frequency systems.
Sciatica treatment options compared
| Treatment |
Best for |
Typical relief |
| Physical therapy + NSAIDs |
Acute sciatica < 6 weeks |
~80% recover |
| Transforaminal epidural |
Sciatica from disc herniation |
Weeks to 12 months |
| Pulsed RF at DRG |
Recurrent radicular pain |
6–18 months |
| Piriformis injection |
Piriformis syndrome |
Weeks to months |
| SI joint injection / RFA |
SI joint dysfunction |
3–12 months |
| Peripheral nerve stimulation |
Focal sciatic neuralgia |
Long-term |
| Spinal cord stimulation |
FBSS, refractory radiculopathy |
Long-term |
| Microdiscectomy |
Severe disc herniation, weakness |
Faster immediate relief |
Where to be seen in DFW
Frequently asked questions about sciatica
How do I know if my sciatica is from a herniated disc?
Disc-related sciatica typically follows a specific nerve distribution — for L5 it’s down the side of the calf and into the top of the foot; for S1 it’s down the back of the calf and into the heel. Clinical exam plus MRI usually confirms it.
Do epidural steroid injections actually work for sciatica?
Yes — a 2025 systematic review of 72 RCTs and 7,701 patients
demonstrated significant pain and function improvement, particularly with transforaminal injections performed under image guidance. Effects can last up to 12 months in responders.
How many injections can I have?
Typically up to 3 in a 6–12 month period, depending on the patient and the response. If injections aren’t producing meaningful relief, repeating them indefinitely is not the answer — we shift to another approach.
Will I need surgery?
Most patients don’t. Surgery is the right call for progressive weakness, intractable pain that fails comprehensive interventional care, or signs of cauda equina syndrome. Otherwise, we exhaust minimally invasive options first.
Do you accept my insurance?
Most major commercial plans, Medicare, Medicaid, MVA, and Texas workers’ comp. We verify benefits when you call (214) 306-4116.
How quickly can I be seen?
Same-week appointments are typical at both DFW clinics.
Related articles from SEVA Healthcare
Take the next step
See a sciatica specialist in Dallas-Fort Worth this week
Dr. Mirchandani and the SEVA Healthcare team will give you a real diagnosis — not just “sciatica.” Same-week consultations at Lewisville and Rowlett.
TX: (214) 306-4116 · sevahealthcare.com
Informational only; not medical advice. Written by Dr. Amit Mirchandani, MD. Medically reviewed by Dr. Jayen Patel, MD. Last updated May 19, 2026.