AM
Dr. Amit Mirchandani, MD
Double Board-Certified Anesthesiology & Pain Medicine · SEVA Healthcare
14 min read
Key Takeaways
- Knee replacement surgery is a great procedure for the right patient at the right time — but many Dallas patients are sent there before minimally invasive alternatives
have been fully explored.
- Genicular artery embolization (GAE)
is the newest of these. A 2024 prospective IDE trial
showed sustained pain relief at 2 years
in moderate-to-severe knee osteoarthritis.
- Genicular nerve radiofrequency ablation (RFA)
can disable the small pain-carrying nerves around the knee and provide 9–18 months of relief, often delaying or avoiding surgery.
- PRP and joint injections
have the longest track record for mild-to-moderate disease; they don’t cure arthritis but can extend the time before more invasive options are needed.
- SEVA Healthcare offers all of these at Lewisville
and Rowlett
— same-week appointments.
If an orthopedic surgeon in Dallas has told you it’s time for a total knee replacement — or if your knee arthritis is bad enough that you’re thinking about it on your own — you should know that the landscape of non-surgical options has changed dramatically in the past three years.
This guide explains what actually causes knee arthritis pain, why pain doesn’t always match the X-ray, and what minimally invasive treatments can do for patients in Dallas, Lewisville, Plano, Frisco, Rowlett, and across the DFW metroplex. Knee replacement is the right choice for some patients; for many others, it’s not the right choice yet.
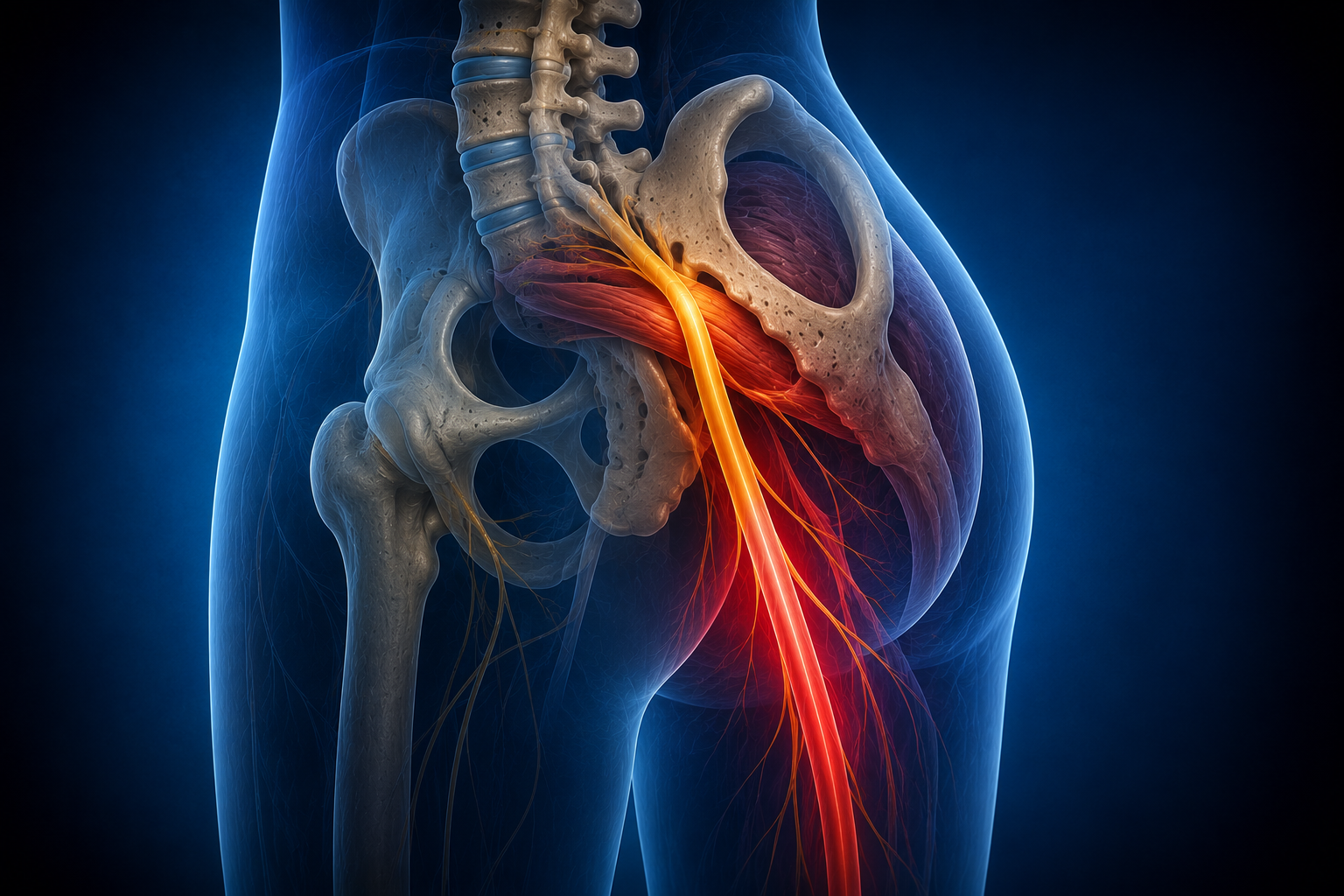
Why knee arthritis hurts — and why imaging doesn’t tell the whole story
Most knee arthritis pain isn’t just “bone on bone.” The real pain generators are usually:
- Inflamed synovial lining
— chronic inflammation in the joint produces ongoing pain signals.
- Hyperactive small arteries
— abnormal blood vessels grow into the inflamed synovium, perpetuating the inflammatory cycle. This is the target of GAE.
- Genicular nerves
— the small sensory nerves around the knee that carry the pain signal upward.
- Cartilage loss + bone-on-bone contact
— real, but often a smaller part of the pain story than X-rays suggest.
- Muscle and ligament dysfunction
from years of guarding and compensation.
Honest note from Dr. Mirchandani
I see Dallas patients regularly whose knee X-rays look terrible but who have manageable pain — and others whose X-rays look mild but who can’t sleep. The pain isn’t in the image. It’s in the inflammation and the nerve signaling. That’s exactly what minimally invasive treatment targets.
Five minimally invasive alternatives to knee replacement
1
Genicular Artery Embolization (GAE)
A minimally invasive procedure performed by an interventional radiologist or interventional pain specialist. Through a small puncture in the upper leg, tiny microspheres are delivered into the abnormal arteries feeding the inflamed knee lining. This reduces inflammation and pain. A 2024 prospective IDE trial published in JVIR
reported sustained symptom relief at 24 months with an acceptable safety profile in patients with moderate-to-severe knee OA. Best for:
Patients with documented knee arthritis pain who haven’t responded to injections, want to delay or avoid replacement, or are not surgical candidates. Read more on our GAE guide.
2
Genicular Nerve Radiofrequency Ablation (RFA)
An outpatient procedure that uses controlled radio waves to disable the small sensory nerves carrying pain signals away from the knee. We confirm the target nerves with diagnostic blocks first; if those blocks produce strong (even if brief) relief, RFA can extend that relief for 9–18 months. Best for:
Patients with knee arthritis pain who responded to a genicular nerve block. Often used as a bridge to delay replacement, or as long-term management for patients who can’t have surgery.
3
Platelet-Rich Plasma (PRP) Therapy
Concentrated growth factors and platelets from your own blood are injected into the knee joint to reduce inflammation and support tissue health. PRP has been studied extensively over the past decade. Best for:
Mild-to-moderate knee arthritis, early degenerative changes, or patients who want a regenerative approach before more invasive options. Several treatments may be needed; results vary by patient and disease severity.
4
Image-Guided Corticosteroid & Hyaluronic Acid Injections
The longest-established option. Steroid injections reduce inflammation rapidly; hyaluronic acid (“gel”) injections add lubrication and may extend the comfortable interval. We perform all of these under ultrasound guidance for accuracy. Best for:
Acute flares or moderate disease while you decide on a longer-term plan.
5
Peripheral Nerve Stimulation (PNS)
A small device placed near the genicular nerves delivers gentle electrical signals to interrupt pain transmission. Useful for select patients with severe knee pain — particularly those with persistent pain after knee replacement, or where surgery isn’t an option. Best for:
Refractory knee pain or post-surgical knee pain.
Side-by-side: knee replacement vs. minimally invasive options
| Option |
Recovery |
Best candidates |
| Total knee replacement |
6–12 weeks intensive, 1 year full |
Severe OA, bone-on-bone, surgical fitness |
| GAE |
Days |
Moderate-severe OA, surgery deferred |
| Genicular RFA |
Days |
Responded to genicular nerve block |
| PRP |
Same day |
Mild-moderate OA, regenerative preference |
| Steroid / HA injection |
Same day |
Acute flare or moderate disease |
| PNS |
Days |
Refractory or post-surgical knee pain |
When knee replacement is still the right answer
There are clear cases where surgery is the right move:
- Severe end-stage osteoarthritis with significant deformity (varus or valgus >15°).
- Pain that has failed comprehensive interventional and rehabilitative care.
- Severe functional limitation — unable to walk a block, climb a single flight of stairs, or sleep through the night.
- Patient is medically fit for surgery and motivated to do post-op rehab.
For these patients, a well-executed total knee replacement is one of the highest-satisfaction procedures in medicine. The point of this article isn’t to argue against replacement — it’s to make sure you have exhausted the right alternatives first.
Where to be seen in Dallas
Frequently asked questions
Can GAE actually delay or replace knee surgery?
For many patients, yes — at least for a meaningful time. The 2024 IDE trial published in JVIR showed sustained 2-year relief in moderate-to-severe knee OA. GAE doesn’t restore cartilage, but it can substantially reduce the pain-driving inflammation in the joint.
Is GAE covered by insurance?
Coverage is improving but still varies by plan. We verify benefits before scheduling and obtain prior authorization when required.
How long does genicular RFA last?
Typically 9–18 months. The procedure can be repeated when pain returns. Many patients use RFA as a bridge while continuing to evaluate replacement timing.
Will PRP regenerate my cartilage?
No treatment regenerates significant cartilage in advanced osteoarthritis. PRP reduces inflammation and may slow degenerative progression. The expectation should be pain reduction and functional improvement, not cartilage restoration.
Do I need an MRI before treatment?
Not always. Standing knee X-rays plus a thorough exam are often enough to make a plan. MRI may be needed for specific questions like meniscus tears or post-surgical anatomy.
Can I have these procedures if I’m on blood thinners?
Most patients on blood thinners can still have these procedures, sometimes with brief medication adjustment. We coordinate with your prescribing physician.
How quickly can I be seen?
Same-week appointments are typical at both DFW clinics.
Related articles from SEVA Healthcare
Take the next step
Explore knee replacement alternatives in Dallas
Dr. Mirchandani and the SEVA Healthcare team will review your imaging, your prior treatments, and your goals — and tell you honestly which options make sense for you.
TX: (214) 306-4116 · sevahealthcare.com
Informational only; not medical advice. Written by Dr. Amit Mirchandani, MD. Medically reviewed by Dr. Jayen Patel, MD. Last updated May 19, 2026.